
April 18 2017
Patellofemoral pain can be like German sausages…… it’s the wurst……..!
Bad jokes aside, this is a common condition that presents to physiotherapy clinics the world over. Here is our take on managing it effectively.
Let’s get the anatomy sorted at the top. First things first, your knee is made up of two joints!
Your tibiofemoral joint consists of, wait for it, your tibia (shin bone) and your femur (thigh bone) and provides the bending and straightening or flexion and extension in your knee.
The other joint is the one in question today, the patellofemoral joint. It comprises the patella (knee cap) and the femur. Hopefully the figure below explains this well;
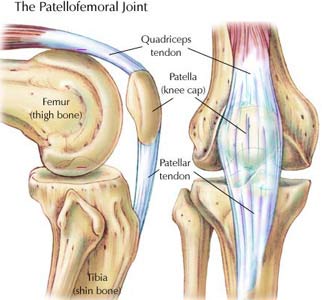
Photo courtesy of askthetrainer.com
The patellofemoral joint is said to be the most common cause of knee pain and it is estimated to affect between 5 – 10% of the population. The pain can be very debilitating and affect everyday activities as well as sporting participation and performance for years if not managed well.
Patellofemoral pain can be a frustrating condition to diagnose for a number of reasons. In fact, there are more names used for patellofemoral pain than there are AFL premierships in South Australia!! You may have had your knee pain called;
- Patellofemoral pain syndrome
- Chondromalacia Patellae
- Anterior Knee Pain
- Anterior Knee Syndrome
- Runner’s Knee
- OR our favourite…….. My Dodgy Old Knee!!
In a recent consensus statement, released by a panel of international experts, it was decided that the term “patellofemoral pain” was the preferred terminology for the condition. So even though it may be in your dodgy old knee that’s what we will call it at Mitcham Rehab!
DIAGNOSING PATELLOFEMORAL PAIN
There are a number of signs and symptoms that can present with patellofemoral pain. Put simply, you have patellofemoral pain if there is;
Pain around or behind your patella that is aggravated by at least one activity that loads the patellofemoral joint on a flexed (bent) knee during a weight bearing activity.
You can also have crepitus (a grinding sensation in the joint when you bend your knee), tenderness to touch around your patella, a small amount of swelling around your patella or pain with sitting, rising from sitting or straightening the knee following sitting.
Although having your knee assessed by several tests that can be done to help diagnose patellofemoral pain no one test can be definitive over any other. Most commonly, 80% of people with patellofemoral pain will have pain with squatting maneuvers and up to 75% will have tenderness to touch around the borders of the patella.
Diagnosis is important in all conditions and cases of patellofemoral pain are no exception. If the condition is left untreated or poorly managed the joint can become osteoarthritic. The best management for arthritic joints (including how learning to play the flute can help…) is written in our osteoarthritis blog here.
TREATMENT FOR PATELLOFEMORAL PAIN
The part you have all been waiting for!!
The consensus statement that was mentioned earlier has suggested a number of key recommendations in the treatment of patellofemoral pain that we will go over.
EXERCISE AS TREATMENT
One of the first things to note is that, like most of our blogs suggest, EXERCISE is a key component!!
A combination of hip and knee exercises are essential for decreasing pain and improving function in patellofemoral pain in the short, medium and long term. People with patellofemoral pain often have weak and poorly functioning thigh and hip muscles. There is some thought that this weakness may be why the condition develops in the first place. It is also thought that due to pain in your knee, you change the way you move which can exacerbate the condition further. Often people with patellofemoral pain bend their knee less with stairs and squatting movements. Due to weakened and overloaded hip muscles the knee also falls in towards the midline of your body which can affect the tracking of the patella in the groove it sits in on the femur which can increase pain and dysfunction further.
The key to overcoming this is a progressive, individualized strengthening program that often starts with exercises in sitting or lying that are pain free. Eventually the exercises will build to involve standing and functional tasks that incorporate both the hip and knee muscles together. Any biomechanical issues will also be retrained as strength and function improves to minimize any influence they are having on contributing to ongoing pain.
One key factor is to understand that the longer the pain has been present, the longer the rehabilitation will take. If the pain has been persistent for years then it could be a gradually increasing program over 12 months that is required to improve. If managed well, the exercises are used as an ongoing preventative program to keep further bouts of knee pain at bay.
PATELLA TAPING
Taping is a complex beast! There are many types of tape (rigid, stretchy, white under wrap, skin coloured, fluoro pink, skull and crossbones pictures!) and there are many ways of applying it. There is some evidence that suggests taping can improve pain in the short term when used in conjunction with exercise. The video below shows one way that taping can help for patellofemoral pain. This is highly individual and best if applied by a physiotherapist initially to then guide people through how to apply it effectively.
ORTHOTICS
In the early stages of the condition, pain is the main presenting problem for most people and orthotics can be a useful intervention for short term pain relief. It has been suggested that 1 in 4 people are likely to benefit from the use of orthotics. Again, a careful assessment by a physiotherapist, or our Podiatrist Guru Craig Douglass, will be able to guide each individual case.
SURGERY
At the present time, the best research evidence available suggests that surgery for patellofemoral pain is not effective. It should only be explored as a last resort if all conservative managements including exercise and activity modification have failed. A careful approach needs to be taken as there can be other underlying causes and in individual assessment and treatment approach is needed in all circumstances.
THE LAST WORD
The final thing to say around this condition is that although exercise is the key to improving pain and function, it needs to be progressed slowly to avoid doing too much too soon.
Often patellofemoral pain arises from people doing too much too soon in the first place. Often in order to get fit, prepare for a fun run or ride or just get the beach body ready for summer! This is great but needs to be done gradually. As a general rule, progress your exercise program by 10% per week and if your pain increases for more than 24 hours post exercise then it may be too much loading for what the tissues can currently handle.
With a gradually progressed exercise program, perhaps some taping or orthotics and the knowledge of how to manage the pain in your not so “dodgy old knee”, everyone should, in time, be able to get on top of this condition.
Maybe it’s not the wurst after all .…!
REFERENCES AND FURTHER READING
If you want to read more on patellofemoral pain;
- A great blog by the team at La Trobe University with videos on one way to tape a knee…. Click here
- An amazing story of Rhys and his journey to pain free knees after 10 surgeries …. Click here
- Patellofemoral Pain Consensus Statement – Part 1 …. Click here
- Patellofemoral Pain Consensus Statement – Part 2 …. Click here
Please call us if this sounds familiar to you or you need help with any other pain or condition. We would love to help. Happy reading until next time!!